CASE REPORT |
https://doi.org/10.5005/jp-journals-10005-2412 |
A Rare Gingival Lesion in Children: Fibroepithelial Hyperplasia
1Department of Pediatric & Preventive Dentistry, Rishiraj college of Dental Science, Bhopal, Madhya Pradesh, India
2Department of Pediatric and Preventive Dentistry, College of Dental Sciences, Karad, Maharashtra, India
3Department of Periodontology, People’s College of Dental Sciences & Research Centre, Bhopal, Madhya Pradesh, India
4Department of Pediatric & Preventive Dentistry, Index Institute of Dental Sciences, Indore, Madhya Pradesh, India
5Department of Orthodontics, People’s College of Dental Sciences & Research Centre, Bhopal, Madhya Pradesh, India
6Department of Pediatric & Preventive Dentistry, People’s College of Dental Sciences & Research Centre, Bhopal, Madhya Pradesh, India
Corresponding Author: Babita Niranjan, Department of Pediatric & Preventive Dentistry, Rishiraj college of Dental Science, Bhopal, Madhya Pradesh, India, Phone: +91 9893079353, e-mail: dr.babitaniranjan@gmail.com
ABSTRACT
Aim and objective: This case report aims to describe the management of a case of rare gingival lesion in a young pediatric patient.
Background: An increase in the size of the gingival tissue is known as gingival hyperplasia. This can cause esthetic as well as functional problems, and interfere with normal functions like mastication and speech. A histological form of fibroma, fibroepithelial hyperplasia is a proliferative fibrous lesion of the gingival tissue. These lesions can be caused by trauma or persistent irritation, or they can develop from the periodontal, periodontal ligament, or periosteum cells.
Case description: This paper discusses a situation in which the parents of a 4-year-old girl presented to the department with a major complaint of swelling in the upper front tooth region, who was diagnosed with fibroepithelial hyperplasia with the help of a biopsy and histologic evaluation.
Conclusion: In this case surgical excision was performed under local anesthesia with no postoperative complications, and a 2-year follow-up was made with a positive outcome.
Clinical significance: When these type of gingival lesions are present, they should be investigated and diagnosed properly. They should be managed as soon as possible without causing any further complications to permanent dentition.
How to cite this article: Niranjan B, Shashikiran ND, Dubey A, et al. A Rare Gingival Lesion in Children: Fibroepithelial Hyperplasia. Int J Clin Pediatr Dent 2022;15(4):468-471.
Source of support: Nil
Conflict of interest: None
Keywords: Fibrous growth, Gingival lesion, Hyperplasia.
INTRODUCTION
Parents are frequently concerned about any unpleasant “lumps and bumps” that appear in their children’s mouths. Pediatricians are in a unique position to detect intraoral tissues in children at a young age, as parents frequently seek their advice in order to ensure their child’s appropriate growth and development.1 However, because the oral cavity is constantly exposed to external and internal stimuli, it shows a wide range of diseases, from developmental to reactive to inflammatory to neoplastic. These lesions might be generalized or limited in nature. Reactive lesions are non-neoplastic nodular swellings that develop in response to chronic and recurring tissue injury that stimulates an exuberant or excessive tissue response. They are clinically and histologically non-neoplastic.2 Pyogenic granuloma, peripheral giant cell granuloma, fibrous hyperplasia, and peripheral fibroma with calcification are the four types of reactive gingival lesions defined by Kfir et al.3
Daley et al. proposed that the word “focal fibrous hyperplasia,” which suggests a reactive tissue response, be used instead of “fibroma,” which implies a benign neoplastic proliferative fibrous connective tissue, which is wrong. It is the most prevalent oral mucosal mass in adults, accounting for roughly 1.2% of the population.4,5 Biopsy should be used to rule out benign tumors (neurofibroma, neurilemmoma, cellular gland tumor, salivary gland tumor, and lipoma) and mucocele as differential diagnoses for these lesions.6
Oral mucosal diseases in children have been reported in a small number of cases. This case report describes an unusual example of a 4-year-old female with fibroepithelial hyperplasia on histopathological examination.
CASE DESCRIPTION
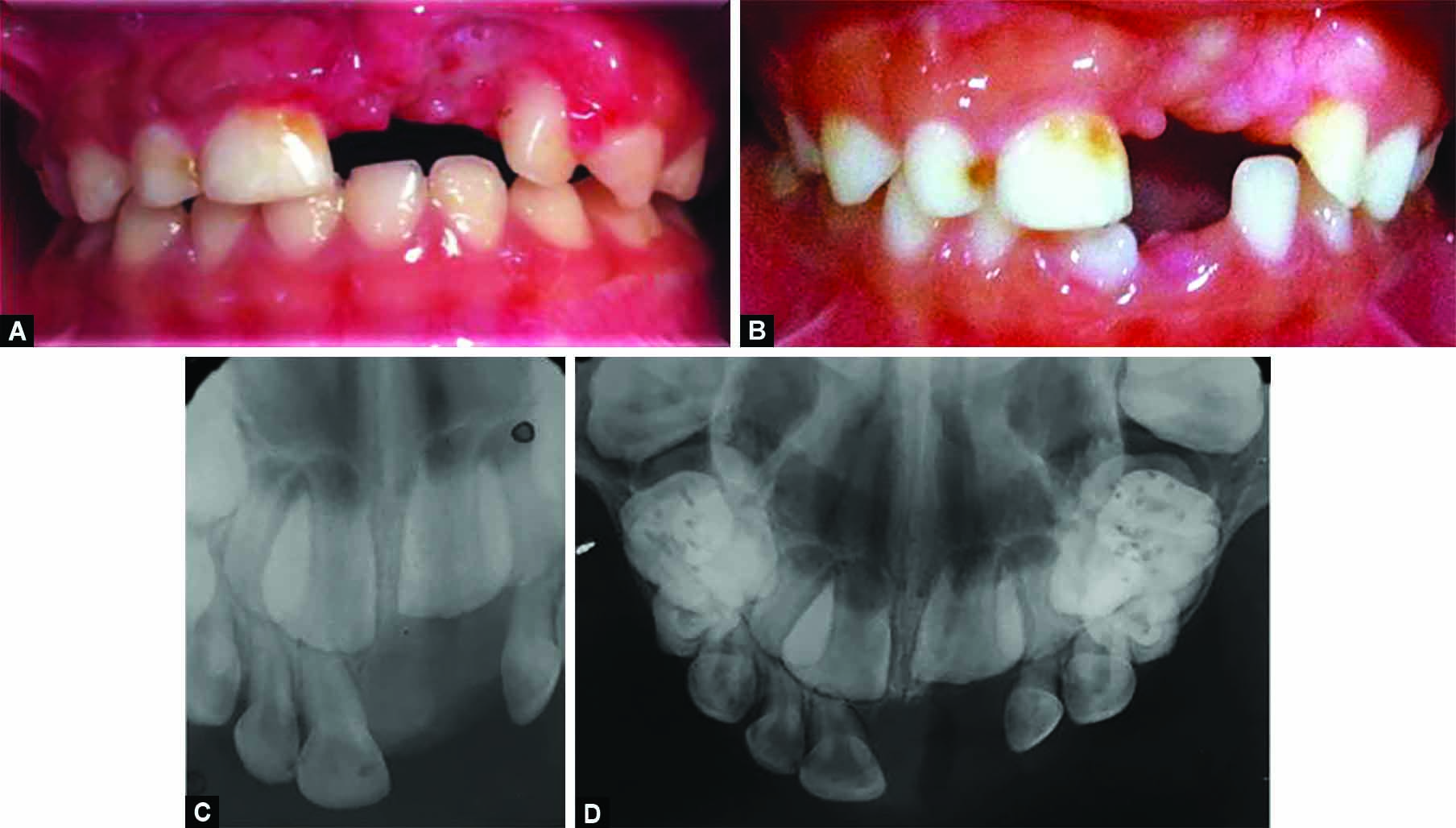
A 4-year-old female child reported to the department of pediatric dentistry with a chief complaint of swelling in the upper front region of the oral cavity for 8 months. The parents of the child gave a history of trauma to the upper anterior teeth region due to a fall on the floor at the age of 3 years. They noticed swelling past 8 months, which gradually increased to attain the present size. Medical history and past dental history revealed no contraindications. Intraoral examination revealed localized, pedunculated, soft, nontender, pinkish color enlargement involving the upper left anterior buccal region of the oral cavity. The swelling extends from the mesial region of 51 to the mesial region of 63 in the buccal and palatal region, involving marginal and interdental gingival, which was 1.5 cm in length and 2 cm in width (Figs 1A and B). This is associated with a buccal shift in 61 and full covering of the crown of 62. A preoperative intraoral periapical and occlusal radiograph was taken and showed displacement of the left primary central incisor (Figs 1C and D). The treatment plan called for a thorough surgical excision of the lesion because of the size of the swelling. Excision of the soft tissue mass and extraction of 61 were performed under local anesthesia, the wound was sutured with a 3-0 black silk suture, and a Coe-Pak was placed. After 7 days, the patient was summoned back for suture removal, and a histopathological analysis of the excised tissue (Fig. 2A) was performed.

Figs 1A to D: (A and B) Intraoral photographs showing gingival hyperplasia extending from mesial surface of 51 to mesial surface of 63; (C) Preoperative intraoral periapical radiograph; (D) Preoperative occlusal radiograph showing hyperplasia with a displacement of left primary central incisor

Figs 2A and B: (A) Excised tissue and extracted right maxillary primary central incisor, which was placed in formalin; (B) Hyperplastic, stratified squamous epithelium with elongated rete ridges into underlying connective tissue stroma
Histopathological Examination
It revealed the presence of hyperplastic parakeratinized stratified squamous epithelium, and basal cells appeared to be hyperchromatic with elongated rete ridges. Connective tissue stroma was fibrocellular, dense inflammatory cells with extravasated red blood cells, and blood vessels were seen (Fig. 2B). On the basis of this histopathological finding, a confirmatory diagnosis of fibroepithelial hyperplasia was made.
The patient was recalled after 1 week; the excised site had healed (Fig. 3A). A 2-year follow-up was done, which showed eruption of permanent right lower incisor and satisfactory result (Figs 3B to D).
Figs 3A to D: (A and B) Postoperative intraoral periapical and occlusal radiograph at 1-week and 2-year follow-up, respectively; (C and D) Intraoral periapical and occlusal radiograph at 2-year follow-up
DISCUSSION
Any pathologic growth that protrudes above the usual contour of the oral surface is referred to as a soft tissue tumor-like lesion.7 The formation of these soft tissue tumor-like lesions in the oral cavity could be caused by a number of different causes. Reactive hyperplasia and neoplasia are the most typical mechanisms at work. The majority of oral mucosa overgrowths are reactive rather than malignant.8 Fibroepithelial hyperplasia is a reactive inflammatory condition that develops in the gingiva and can manifest as a range of lesions depending on the clinical presentation.9
Oral practices such as lip biting/sucking in childhood have been linked to a few oral diseases, such as irritant fibroma, according to the literature.10 In a 4 year and 6-month-old infant, a rare relationship of reactive hyperplasia or traumatic fibroma with a natal tooth was reported.11
Few researches have been reported on the occurrence of oral soft tissue lesions in children in detail. In a total of 260 cases, Pour et al.8 found that 0.38% were diagnosed histologically with irritant fibroma.
In the oral cavity, fibroma is the most prevalent benign soft tissue tumor. The majority of fibromas are reactive localized fibrous hyperplasia caused by trauma or local irritation in the clinical setting. In contrast to neoplasia, hyperplasia is a self-limiting process, and hyperplastic cells may retreat if the stimulus is removed.9 Lesions such as giant cell fibroma, neurofibroma, peripheral giant cell granuloma, mucocele, lipoma, or salivary gland tumor are included in the differential diagnosis of epithelial hyperplasia.12
Fibrous inflammatory hyperplasia can manifest itself clinically as pedunculated or sessile development on any surface of the oral mucous membrane. A pedunculated growth was seen in the present case report, which was removed under local anesthetic and sent for histological examination, which confirmed the diagnosis of fibroepithelial hyperplasia. These lesions have hyperplastic stratified squamous epithelium with slender finger-like rete ridges extending into the fibrocellular connective tissue stroma. There is also infiltration of chronic inflammatory cells. Complete local excision is used to treat these lesions, and a low rate of recurrence is expected. Similar findings were reported in the present case. A 2-year follow-up showed a satisfactory result.
CONCLUSION
Diversity in a group of pathologic lesions present in the oral cavity often presents a diagnostic challenge to many clinicians. With the help of histopathological examination, such lesions can be identified and properly diagnosed. Focal fibrous hyperplasia, giant cell fibroma, mucocele, and epulis are the most frequent oral lesions. The present case report is an attempt to describe an unusual finding of oral lesions, which is rare in pediatric patients. A histopathology report will ensure that the patient receives a better and more appropriate treatment plan and that the lesions do not reoccur.
Clinical significance
Clear differentiation between hyperplasia and neoplasia needs to be understood by clinicians, as neoplasias are long-standing hyperplastic lesions in the presence of chronic irritation that can get converted to neoplasia and not self-limiting conditions. These lesions are most commonly reported in adults, but there is less published literature on pediatric patients.
In addition to the physical characteristics of the lesion, the patient’s demographics, presence of associated symptoms, and location of the lesion and histopathologic architecture all give clues to make an adequate and appropriate diagnosis.
REFERENCES
1. American Academy of Pediatric Dentistry reference manual. Oral health policies. Pediatr Dent 2004;26(7 Suppl):14–61.
2. Cotran R, Kumar V, Collins T. Robbins Pathologic Basis of Disease. 6th ed. W.B. Saunders; 1999.
3. Kfir Y, Buchner A, Hansen LS. Reactive lesions of the gingiva. A clinicopathological study of 741 cases. J Periodontol 1980;51(11):655–661. DOI: 10.1902/jop.1980.51.11.655
4. Daley TD, Wysocki GP, Wysocki PD, et al. The major epulides: clinico pathological correlations. J Can Dent Assoc 1990;56(7):627–630.
5. Buchner A, Calderon S, Ramon Y. Localized hyperplastic lesions of the gingival: a clinicopathological study of 302 lesions. J Periodontol 1977;48(2):101–104. DOI: 10.1902/jop.1977.48.2.101
6. Esmeili T, Lozada-Nur F, Epstein J. Common benign oral tissue masses. Dent Clin North Am 2005;49(1):223–240. DOI: 10.1016/j.cden.2004.07.001
7. Delaney JE, Keels MA. Pediatric oral pathology: soft tissue and periodontal conditions. Paediatr Clin North Am 2000;47(5):1125–1147. DOI: 10.1016/s0031-3955(05)70260-1
8. Pour MA, Rad M, Mojtahedi A. A survey of soft tissue tumor-like lesions of oral cavity: a clinicopathological study. Iran J Pathol 2008;3(2):81–87.
9. Shafer, Hine, Levy. Benign and malignant tumors of oral cavity. Shafer’s Textbook of Oral Pathology. 5th ed. New Delhi: Elsevier; 2007. p. 178–180.
10. Barberia E, Lucavechi T, Cardenas D, et al. An atypical lingual lesion resulting from the unhealthy habit of sucking the lower lip: a clinical case study. J Clin Pediatr Dent 2006;30(4):280–282. DOI: 10.17796/jcpd.30.4.p20272221365477w
11. Singh S, Subbareddy VV, Dhananjaya G, et al. Reactive fibrous hyperplasia associated with a natal tooth. J Indian Soc Pedo Prev Dent 2004;22(4):183–186.
12. Buchner A, Sandbank M. Multiple fibroepithelial hyperplasias of the oral mucosa. Oral Surg Oral Med Oral Path 1978;46(1):34–39. DOI: 10.1016/0030-4220(78)90434-6
________________________
© The Author(s). 2022 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted use, distribution, and non-commercial reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.