RESEARCH ARTICLE |
https://doi.org/10.5005/jp-journals-10005-2127 |
Transportation and Centering Ability of Kedo-S Pediatric and Mtwo Instruments in Primary Teeth: A Cone-beam ComputedTomography Study
1,3Department of Pediatric and Preventive Dentistry, Faculty of Dental Sciences, Sri Ramachandra Institute of Higher Education and Research (Deemed to be University), Chennai, Tamil Nadu, India
2SR Specialty Dentistry, Chennai, Tamil Nadu, India
Corresponding Author: Kavitha Swaminathan, Department of Pediatric and Preventive Dentistry, Faculty of Dental Sciences, Sri Ramachandra Institute of Higher Education and Research (Deemed to be University), Chennai, Tamil Nadu, India, Phone: +91 4424768027, e- mail: kadva28@gmail.com
ABSTRACT
Background: Cleaning and debriding the canals and preserving the shape of the canal without deformation is the primary goals of pulpectomy. Transportation is a critical endodontic iatrogenic fault that could cause a catastrophe. This study evaluated the canal centering ability and canal transportation caused by Kedo-S pediatric and Mtwo instruments, using a cone-beam computed tomography (CBCT).
Materials and methods: This in vitro study was performed on distal roots of 50 primary mandibular first molars. The teeth were scanned using CBCT and randomly divided into two groups. The canals were then prepared using either Kedo-S or Mtwo files ( n = 25). The instrumented canals were rescanned. The scanned volumes were sectioned at 2, 4, and 6 mm from cementoenamel junction (CEJ). Canal transportation (CT) and instrument centering ability were estimated and compared in both groups.
Results: The mean values for two study groups were compared. T -test was used to determine theP value. The Levene’s test was used to test the significance between two groups. The two groups showed similar results in terms of transportation and centering ability (P > 0.05).
Conclusion: Kedo-S pediatric and Mtwo instruments demonstrated similar canal centering ability and CTs.
How to cite this article: Haridoss S, Rakkesh KM, Swaminathan K. Transportation and Centering Ability of Kedo-S Pediatric and Mtwo Instruments in Primary Teeth: A Cone-beam Computed Tomography Study. Int J Clin Pediatr Dent 2022;15(S-1):S30-S34.
Source of support: Nil
Conflict of interest: None
Keywords: Canal centering ability, Canal transportation, Kedo-S instrument, Primary teeth, Root canal preparation, Pediatric rotary files
INTRODUCTION
Primary teeth with extensive caries involving pulp are indicated for a pulpectomy procedure. Traditionally pulpectomy was performed by stainless steel hand files.1 Several NiTi rotary files were later introduced with improved shaping abilities to reduce the risk of technical errors.2 The Mtwo system which consists of four instruments with variable tip sizes. It should be used without early coronal enlargement, suggested by the manufacturer, in single-length techniques.3-5 To perform an effective pulpectomy in primary teeth, it is mandatory to use rotary files with customized length, taper, and tip size that is suitable for root canal morphology of primary teeth.6 The Kedo-S rotary file (pediatric rotary system) is a file system with a length of 16 mm and the working area (cutting flutes) being 12 mm. These files have variable varying taper (4-8%).7 Cone-beam computed tomography is widely used for evaluating improvements in the root canal anatomy and visualization of maxillofacial hard tissues regions. Cone-beam computed tomography images provide submillimeter resolution with 15 times smaller than traditional scans with high quality and quick scanning time (10-70 seconds).8 Based on the literature search there is a lack of in vitro studies comparing Kedo-S with other NiTi rotary files. Evidence shows that Mtwo file maintains centering ability and shows better removal of debris from even in curved canals compared to other rotary systems.9,10 Hence this study is intended to evaluate the CT and centering ability of Kedo-S and Mtwo files using CBCT.
MATERIALS AND METHODS
Selection and Preparation of Samples
Fifty extracted human mandibular primary first molars with minimum of 7 mm root length were collected and stored in formalin. The study was conducted in the Department of Pediatric and Preventive Dentistry, Sri Ramachandra Faculty of Dental Sciences, Sri Ramachandra Institute of Higher Education and Research with ethical approval from the Institutional Ethical Committee (CSP/17/JUN/59/217). Occupational Safety and Health Administration guidelines and regulations were used for storage and handling of teeth.
All the sample teeth had their crowns cut off horizontally at the level of the CEJ using sectioning disk. The sectioned roots were mounted in a wax block of a standardized dimension. Distal roots of the primary mandibular molar were selected as it is rounded, shorter, and taper more apically.11 Standard access cavities were made for all teeth with a diamond bur (BR 40, MANI, INC, Japan). Preoperative radiographs were taken and canal patency was assessed using 15 root canal instrument .All the samples teeth were then divided into two groups containing 25 teeth each (Flowchart 1).

Flowchart 1: Diagrammatic representation of study design
Canal Preparation
In group I, E1 Kedo-S files with X Smart Endodontic motor (Dentsply Maillefer, Switzerland) were used to prepare the canal with 300 rpm speed and torque of 2.2 N cm. Mtwo Basic Sequence NiTi rotary files (VDW, Munich, Germany) driven by an X Smart Endodontic motor (Dentsply Maillefer, Switzerland) at a speed of 300 rpm and a torque of 1.2 N cm were used for canal preparation in group II. The canals were prepared for the full length by single length technique without early coronal enlargement. Three Mtwo Basic sequence instruments (no.10 size to no. 20 size) were used in primary teeth.
Canals were irrigated with 3 mL of a 5.25% NaOCl solution (27-gauge needle). Glyde (Dentsply, Maillefer) was used for lubrication during instrumentation and after instrumentation; each instrument was changed after five canals.
Specimen Scan
Teeth were scanned before and after canal preparation with CBCT (Planmeca ProMax® 3D Mid) with a field of view = 80 mm × 80 mm and voxel size of 200 mm. The exposure time of 12 seconds and slice thickness of 0.4 mm with 90 kV and 10 mA was used. Romexis® digital imaging software, version 3.5.2 (Planmeca, Helsinki, Finland) were used to assess the CBCT images. The CEJ was taken as a reference point. The canal preparation was measured at three levels.
The cervical level was assessed at 2 mm below the CEJ. The middle level was assessed at 4 mm below CEJ. The apical level was assessed at 6 mm below CEJ.
Canal Transportation
Voxel measurements were used to quantify noninstrumented and instrumented canals, while M1 was used to calculate the number of voxels at the mesial wall of the noninstrumented canal from the outer surface of the mesial portion of the root. M2 was the calculation, after instrumentation, of the number of voxels from the outer root surface of the mesial part of the root to the canal wall. The calculation of the number of voxels from the outer surface of the distal root portion to the distal wall of the noninstrumented canal was D1. D2 was the calculation after instrumentation of the number of voxels from the external surface of the distal portion of the root to the distal surface of the canal (Figs. 1 and 2).
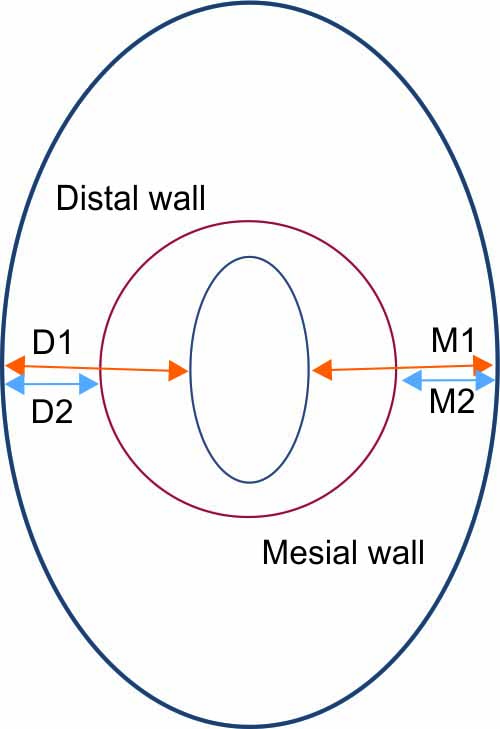
Fig. 1: A schematic diagram, showing the cross section of non-instrumented canal (blue small ovoid) and instrumented canal (red circle)
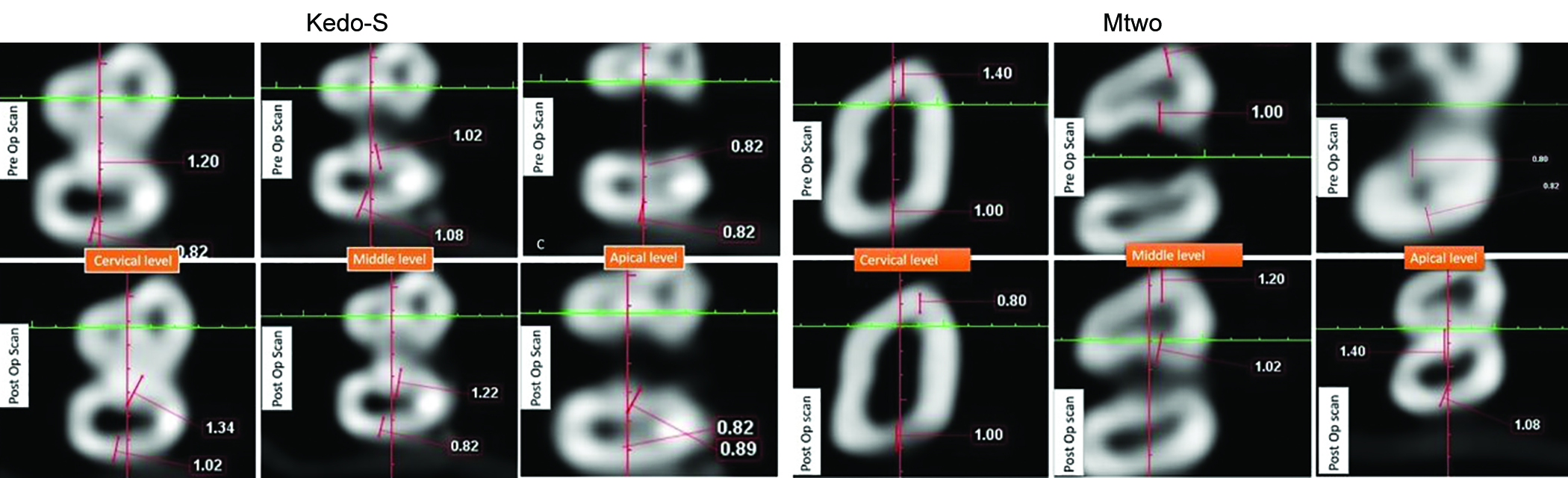
Fig. 2: Representative CBCT scanning images of Kedo-S and Mtwo rotary systems
From the following equation, CT was assessed
(CT) = (M 1 -M 2) -(D 1 -D2)
CT equal to 0 (zero) meant lack of transport as regards the direction of canal transport; negative value indicates transportation to the distal trend and transportation to the mesial trend is indicated by a positive value.12
Canal Centering Ability
The following equation was used to determine the canal centering ability centralization ability ratio = (M 1 − M 2)/(D 1 − D 2)
A result equal to 1.0 demonstrated complete centralization ability ratio. This meant that the instrument had a lesser capacity to sustain itself in the central axis of the canal while this value was closer to zero.12
Statistical Analysis
The mean and standard deviation for canal transportation and canal centering ability were estimated and T -test was used to calculate theP value. Levene’s test was used to calculate the level of significance and was set at 0.05.
RESULTS
In this study, canal transportation and centering ability was examined at 2, 4, and 6 mm from CEJ. The mean CT for the mentioned diameters is listed in Table 1 and Figure 3. There was no considerable difference between the two systems, based on statistical evidence, in terms of canal transportation.
| Groupn | Cervical level (2 mm below CEJ)mean ± SD | Middle level(4 mm below CEJ)mean ± SD | Apical level(6 mm below CEJ)mean ± SD |
|---|---|---|---|
| Group I n = 25 | −0.008 ± 0.18 | −0.031 ± 0.02 | −0.018 ± 0.28 |
| Group II n = 25 | 0.026 ± 0.93 | −0.016 ± 0.09 | −0.09 ± 0.94 |

Figs 3A and B: Distribution of the amount of displacement in the two rotary systems: (A) Kedos-S; (B) Mtwo
The frequency of the direction of transportation is shown in Table 2. In general, transportation to the distal area in both systems was higher than transportation to the mesial area, although it was not a statistically significant difference.
| Distance from CEJ | System | Transportation toward distal (%) | No transportation (%) | Transportation toward Mesial (%) | P value |
|---|---|---|---|---|---|
| Cervical2 mm | Kedo-S | 12 (48) | 9 (36) | 4(16) | 0.489 |
| Mtwo | 7(28) | 14(56) | 4(16) | ||
| Middle4 mm | Kedo -S | 12(48) | 9(36) | 4(16) | 0.746 |
| Mtwo | 11(44) | 12(48) | 2(8) | ||
| Apical4 mm | Kedo-S | 11(44) | 10(40) | 4(16) | 0.882 |
| Mtwo | 11(44) | 13(52) | 1(4) |
value < 0.05 = Statistically significant.P† value, P value = Significant P*
The Kedo-S and Mtwo rotary files maintain the canal centering ability better in the middle level when compared to the cervical and apical levels. Both the files were not statistically significant (P < 0.05) in maintaining the canal centering ability (Table 3).
| Levels | Mean ± SD Kedo-S | Mean ± SD Mtwo | Mean difference Mtwo File vs. Kedo -S file | P value | 95% Confidence interval of the difference | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Cervical 2 mm below CEJ | 0.82 ± 2.12 | 0.26 ± 3.71 | 0.562 | 0.562 | −1.20 | 2.32 |
| Middle 4 mm below CEJ | 0.72 ± 1.84 | 0.93 ± 1.09 | −0.207 | 0.632 | −1.07 | 0.66 |
| Apical 6 mm below CEJ | 1.3 ± 2.16 | 2.45 ± 5.58 | −1.186 | 0.338 | −3.68 | 1.30 |
value <0.05 = Statistically significantP† value, P value = Significant P*
DISCUSSION
The basic principles for biomechanical preparation in endodontic treatment are complete removal of vital tissue, necrotic remnants, debris, and infected dentin thereby render tissue repair and regeneration.13 The root canal geometry is different in primary teeth and hence it is important to assess the canal preparation using different instruments.14 The strength of the nickel-titanium (Ni-Ti) rotary systems was to uniformly, smoothly prepare the curved canals and maintain the shape with less instrument time and canal tapering than hand instruments.15 In the present study, teeth with a least amount 7 mm of root length were selected to simulate a clinical conditions. As it offers accurate three-dimensional (3D) observation, CBCT imaging has been used in measuring dentin thickness removal, canal curvature, transportation, and canal cantering ratio.16 Therefore, the objective of this research was to CBCT evaluation of the transportation and centering ability with rotary files of Kedo-S and Mtwo.
In our study, the Mtwo rotary system shows no transportation at 2, 4, and 6 ,mm. This finding was similar to the results of previous studies that evaluated the preparation of curved canals by using Mtwo files and other NiTi rotary files. It was reported that the Mtwo files conserved canal curvatures better than the K3, race,3,4 and Protaper instruments.17 Owing to the design of Mtwo files, fewer preparation errors have been reported.18 However, no significant difference was noted in this respect between the two systems. Both systems in all sections mostly recorded < 0.1 mm of canal transportation, which is within the clinically acceptable range given by Peters.19
In this study, both the rotary file systems maintain the canal centering ability better in the middle level are in agreement with Selvakumar et al. who observed K3 rotary file (2 and 4% taper) maintain the centering ability better than stainless steel.20On the contrary, Gambil et al. have also found no significant difference between NiTi and K- flex instruments.12
The risk factors for canal transportation and centering ability are complex radicular anatomy, the lack of direct access, instrument design, incorrect sequences of the usage of different instruments, speed of instrument rotation, the use of inadequate irrigation, and lubricant solutions.21 In these risk factors, the instrument design and internal canal morphology are intrinsic factors that are independent of the operator’s expertise and skill. Among these two factors, the instrument design can be modified. In our study, the Kedo-S file shows more distal displacement even though it is not statistically significant by modifying the shape of the instrument might reduce the transportation of the file.
The impediment of this investigation was smarter to compare the outcomes with a conventional stainless steel file. Notwithstanding, transportation has not conceded to the highest quality level.22 Since the lower transportation of NiTi files compared to that of stainless steel hand instruments is already established,23 we focused on recently presented newly introduced pediatric rotary with existing NiTi instruments as they were. Another limitation was that regardless of our endeavor to standardize the samples using the exclusion/inclusion criteria, extracted teeth cannot be completely standardized in terms of canal shapes and sizes.24,25
The quality purposes of our investigation are canal preparation was performed in natural teeth consequently, its outcomes could be better generalizable to the clinical practice. The procedures were performed by one operator (high reproducibility of results), utilizing software calculations (high precision), and utilization of CBCT.
CONCLUSION
Within the restrictions of this study, no difference was noted in canal transportation and centering ability of the rotary files used in this study. Thus, both systems can be used with minimum endangerment of procedural errors in root canal preparation. In terms of canal transportation and centering ability, Kedo-S file would be safer in primary teeth. However, further investigations are needed to evaluate the performance of Kedo-S pediatric files in the uneven walls of primary teeth with larger sample size.
Clinical Significance
The Kedo-S pediatric rotary file showed clinically appropriate transportation and centering ability that can be recognized as major innovations in pediatric endodontics.
REFERENCES
1. Barr ES Kleier DJ Barr NV. Use of nickel-titanium rotary files for root canal preparation in primary teeth. Pediatr Dent 1999;21:453-454. PMID: 10633522.
2. Prabhakar AR Yavagal C Dixit K et al. Reciprocating vs rotary instrumentation in pediatric endodontics: cone beam computed tomographic analysis of deciduous root canals using two single-file systems. Int J Clin Pediatr Dent 2016;9(01):45-49. DOI: 10.5005/jp-journals-10005-1332
3. Schafer E Erler M Dammaschke T. Comparative study on the shaping ability and cleaning efficiency of rotary Mtwo instruments: part 1: shaping ability in simulated curved canals. Int Endod J 2006;39:196-202. DOI: 10.1111/j.1365-2591.2006.01074.x
4. Schafer E Erler M Dammaschke T. Comparative study on the shaping ability and cleaning efficiency of rotary Mtwo instruments: part 2: cleaning effectiveness and shaping ability in severely curved root canals of extracted teeth. Int Endod J 2006;39:203-212. DOI: 10.1111/j.1365-2591.2006.01075.x
5. Kuzekanani M Walsh L Yousefi MA. Cleaning and shaping curved root canals: Mtwo vs Protaper instruments, a lab comparison. Indian J Dent Res 2009;20:268-270. DOI: 10.4103/0970-9290.57355
6. Kuo, Ching I. et al. Application of Ni-Ti Rotary Files for Pulpectomy in Primary Molars. Journal of Dental Sciences. 2006;1:10-15. DOI: 10.30086/JDS.200603.0002
7. Jeevanandan G Govindaraju L. Clinical comparison of Kedo-S paediatric rotary files vs manual instrumentation for root canal preparation in primary molars: a double blinded randomised clinical trial. Eur Arch Paediatr Dent 2018;19(04):273-278. DOI: 10.1007/s40368-018-0356-6
8. Todd R. Cone beam computed tomography updated technology for endodontic diagnosis. Dent Clin North Am 2014;58(3):523-543. DOI: 10.1016/j.cden.2014.03.003
9. Honardar K, Vesal N, Hamze F, et al. A comparison of Mtwo rotary file with K-file on negotiation of second mesiobuccal canal in maxillary first molar: a clinical study. Iran Endod J 2008;3:29-32. DOI: 10.22037/IEJ.V3I2.405
10. Foschi F Nucci C Montebugnoli L et al. SEM evaluation of canal wall dentine following use of Mtwo and ProTaper NiTi rotary instruments. Int Endod J 2004;37(12):832-839. DOI: 10.1111/j.1365-2591.2004.00887.x
11. Ash MM, Nelson SJ. Wheeler’s dental anatomy, physiology and occlusion. 9th ed. Philadelphia, PA: W.B. Saunders; 2009. p. 63.
12. Gambill M Alder M Del Rio E. Comparison of nickel titanium and stainless-steel handfile instrumentation using computed tomography. J Endod 1996;22:369-375. DOI: 10.1016/S0099-2399(96)80221-4
13. Daito M Kawahara S Kato M et al. Radiographic observations on root resorption in the primarydentition. J Osaka Dent Univ 1991;25:1-23. PMID: 1813600.
14. Hidalgo LRDC Silva LABD Leoni GB et al. Mechanical preparation showed superior shaping ability than manual technique in primary molars: a micro-computed tomography study. Braz Dent J 2017;28(04):453-460. DOI: 10.1590/0103-6440201601552
15. Azar MR Mokhtare M. Rotary Mtwo system versus manual K-file instruments: efficacy in preparing primary and permanent molar root canals. Indian J Dent Res 2011;22(02):363. DOI: 10.4103/0970-9290.84283
16. Elsherief SM Zayet MK Hamouda IM. Cone-beam computed tomography analysis of curved root canals after mechanical preparation with three nickel-titanium rotary instruments. J Biomed Res 2013;27(04):326-335. DOI: 10.7555/JBR.27.20130008
17. Sonntag D Ott M Kook K et al. Root canal preparation with the NiTi systems K3, Mtwo and ProTaper. Aust Endod J 2007;33:73-81. DOI: 10.1111/j.1747-4477.2007.00062.x
18. Giovannone T Migliau G Bedini R et al. Shaping outcomes using two Ni-Ti rotary instruments in simulatedcanals. Minerva Stomatol 2008;57:143-154. PMID: 18427359.
19. Peters OA. Current challenges and concepts in the preparation of root canal systems: a review. J Endod 2004;30:559-567. DOI: 10.1097/01.don.0000129039.59003.9d
20. Selvakumar H Anandhan V Thomas E et al. Evaluation of canal transportation and centering ability of K 3 (0.02%) and K 3 (0.04%) with hand K files in primary teeth using spiral computed tomography. J Indian Soc Pedod Prev Dent 2014;32(04):286-291. DOI: 10.4103/0970-4388.140943
21. Karabucak B Gatan AJ Hsiao C et al. A comparison of apical transportation and length control between EndoSequence and Guidance rotary instruments. J Endod 2010;36(01):123-125. DOI: 10.1016/j.joen.2009.09.015
22. Honardar K Assadian H Shahab S et al. Cone-beam computed tomographic assessment of canal centering ability and transportation after preparation with twisted ile and Bio RaCe instrumentation. J Dent (Tehran) 2014;11(04):440-446. Epub 2014 Jul 31. PMID: 25584056; PMCID: PMC4283746.
23. Tharuni SL Parameswaran A Sukumaran VG. A comparison of canal preparation using the K-file and Lightspeed in resin blocks. J Endod 1996;22(09):474-476. DOI: 10.1016/S0099-2399(96)80081-1
24. Khalilak Z Fallahdoost A Dadresanfar B et al. Comparison of extracted teeth and simulated resin blocks on apical canaltransportation. Iran Endod J 2008;3(04):109-112. Epub 2008 Oct 1. PMID: 24082902; PMCID: PMC3782243.
25. Weine FS Kelly RF Lio PJ. The effect of preparation procedures on original canal shape and on apical foramen shape. J Endod. 1975;1(08):255-262. DOI: 10.1016/S0099-2399(75)80037-9
________________________
© The Author(s). 2022 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted use, distribution, and non-commercial reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.